IT'S TIME TO RESTORE
BETTER MENTAL HEALTH
Recovery groups, coaching and learning opportunities
SUPPORTING THOUSANDS EVERY YEAR
Restore has been supporting individuals across Oxfordshire since 1977. People are supported towards their own mental health recovery goals, such as rebuilding confidence and skills, often moving-on to employment, volunteering or training. Members can attend recovery groups weekly for up to two years and receive one-to-one coaching. Restore is also home to Oxfordshire Recovery College for courses that support recovery, and Restore provides workplace mental health training.
500
Individuals in recovery groups
7500
Sessions attended last year
3000
Course attendances a year
39%
Coachees supported into work
87%
Said they felt well-supported
Rebuilding confidence and skills with individuals who have experienced mental ill health.
Restore offers community activities and workplace training to increase knowledge and reduced stigma.
"At Restore I have found support and encouragement. They have made me feel that I do have a value in life. The companionship and contact with others has helped ease the loneliness inherent in suffering from depression and anxiety. The guidance... had been invaluable. Without it, I would be in a much darker place"
MULTI-FACETED APPROACH



"To a very large extent, Restore has given me purpose, helping me to see there is a reason for going on, for continuing the struggle. Forcing me to face and overcome fears... it is a safe space where I am valued and wanted."
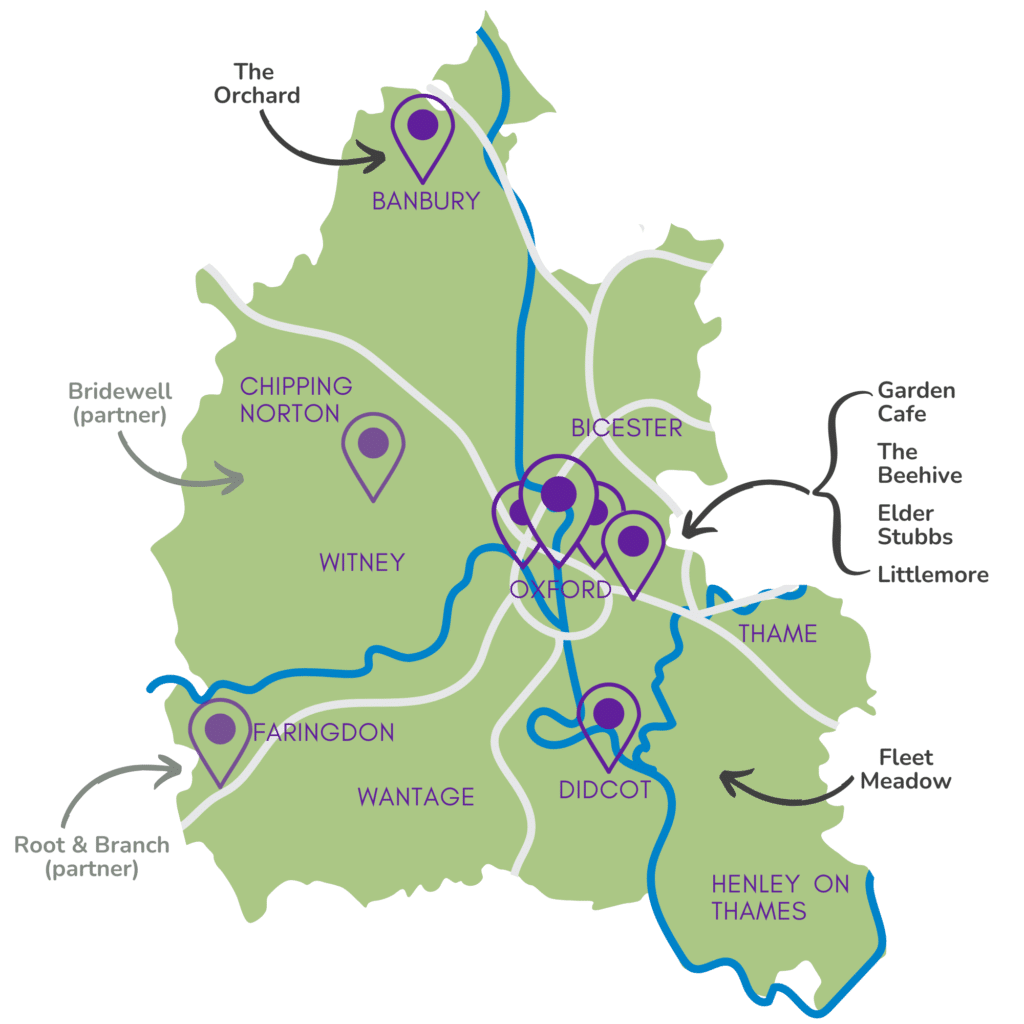
ACROSS OXFORDSHIRE AND ONLINE
Banbury, Didcot, Oxford, and online. Plus two partner sites. Training can be delivered at a external locations.
Head Office
Restore, Manzil Way, Oxford, OX4 1YH
Oxon. Recovery College
Multiple locations
The Orchard
28 Calthorpe St, Banbury, OX16 5EX
Coaching
Multiple locations
Training
Multiple locations
Bridewell (partner)
Walled Garden, Wilcote, OX7 3EB
Garden Cafe
Manzil Way, Oxford, OX4 1YH
The Beehive
Restore, Manzil Way, Oxford, OX4 1YH
Elder Stubbs
Rymers Lane, Oxford, OX4 3DY
Littlemore
Sandford Road, Littlemore, OX4 4XN
Fleet Meadow
Sandringham Rd, Didcot, OX11 8TP
Root & Branch (partner)
Westmill Farm, Watchfield, SN6 8TH











